
Your Gut Is Running Your Hormones...Meet the Estrobolome
Quick answer: The estrobolome is the collection of gut bacteria responsible for regulating estrogen metabolism. When gut microbiome diversity is compromised, estrogen recirculates instead of being excreted—driving hormone imbalances that show up as acne, heavy periods, perimenopausal anxiety, skin aging, and more. Fixing the gut is often the missing step in treating these symptoms.
Most women have been told their labs are "normal." Their periods are heavy, their skin is breaking out along the jawline, they haven't slept past 3AM in six months—but their bloodwork comes back unremarkable. So they leave the clinic with a referral to dermatology, a brochure about stress management, and a quietly mounting suspicion that something is being missed.
Something is being missed. And it lives in your gut.
The estrobolome is a subset of your gut microbiome—a community of bacterial species whose collective enzymatic activity directly regulates how your body processes, recycles, and eliminates estrogen. It's not a fringe concept. It was formally defined in a landmark 2011 paper by Plottel and Blaser in Science Translational Medicine, and the downstream clinical implications have been quietly reshaping integrative medicine ever since. Quietly, because this is not the kind of information that makes it into a 12-minute GP appointment.
This post covers the full picture: how the estrobolome works, what goes wrong across the reproductive lifespan, how it shows up on your skin, and what the evidence actually supports in terms of intervention. Whether you're a patient trying to connect the dots or a clinician looking for a more sophisticated framework, the gut-hormone axis is a conversation worth having—and it's long overdue.
What Is the Estrobolome, and Why Does It Matter?
The estrobolome refers to the aggregate of enteric bacterial genes capable of metabolizing estrogens. In plain terms: your gut bacteria have an opinion about your hormones, and they're not shy about expressing it.
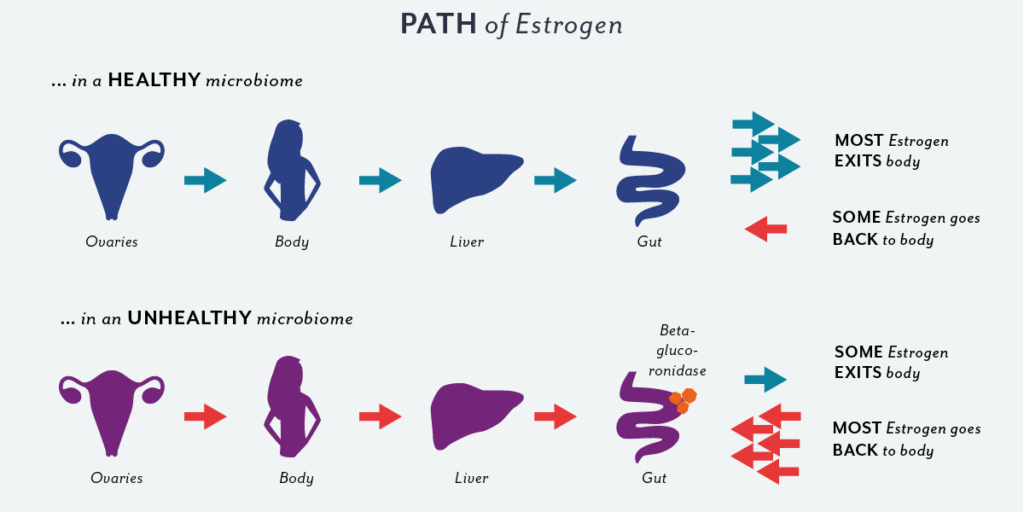
Here's the short version of how it works. The liver detoxifies estrogen by attaching a glucuronide molecule to it—essentially gift-wrapping it for disposal. That package travels through bile into the gut, where it should be excreted. The problem arises when certain gut bacteria produce an enzyme called beta-glucuronidase, which snips the package open. The estrogen is then unwrapped, reactivated, and reabsorbed into circulation through the gut wall. This process is called enterohepatic recirculation, and it's the mechanism by which a dysbiotic gut can effectively override your liver's careful housekeeping.
The result? More estrogen circulating than your labs necessarily captured—or more precisely, more estrogen behaving in ways a single blood draw at a single moment in time won't reveal.
Why "Normal" Labs Don't Tell the Whole Story
Serum estradiol on day 3 of your cycle is a data point, not a diagnosis. It tells you the level of estrogen in your blood at a specific moment. It says nothing about:
- How efficiently your liver is conjugating estrogen for excretion
- What your gut bacteria are doing with it afterward
- Which metabolic pathway your estrogen is taking once it gets there
- What your progesterone-to-estrogen ratio looks like across the full cycle
That last point matters enormously. As Jerilynn Prior's research on progesterone's underappreciated role demonstrated as early as 2005, relative progesterone deficiency—not just absolute estrogen excess—can drive the clinical picture of estrogen dominance (Prior, 2005). Two women can have identical estradiol levels and radically different symptom profiles depending on their progesterone levels, their gut microbiome diversity, and their metabolic pathway preferences.
Medicine has historically treated hormones as a volume problem. The estrobolome reframes it as a systems problem. There's a meaningful difference.
The Estrogen Recirculating Loop: Your Liver Tidies, Your Gut Untidies
To visualize the estrobolome in action, think of your liver as a meticulous packer and your gut as an airport baggage handler who keeps unzipping the suitcase.
The process looks like this:
- Estrogen is used by target tissues throughout the body
- The liver conjugates it—attaching glucuronic acid to flag it for excretion
- Conjugated estrogen enters the gut via bile
- Beta-glucuronidase (produced by bacteria like Escherichia coli, Clostridium, and certain Bacteroides species) cleaves the glucuronide bond
- Free estrogen is reabsorbed into the portal circulation and returns to systemic use
A healthy, diverse microbiome keeps beta-glucuronidase activity in check. A dysbiotic one—depleted by antibiotics, ultra-processed foods, chronic stress, or poor sleep—allows it to run unchecked. The clinical consequence is elevated circulating estrogen relative to what the body intended to clear.
This isn't theoretical. Medicine has already acknowledged it indirectly: the well-documented interaction between antibiotics and oral contraceptives—where antibiotics can reduce OCP efficacy by disrupting the gut bacteria responsible for recycling synthetic ethinyl estradiol—is enterohepatic recirculation in clinical practice. The gut is already recognized as a dial on hormonal activity. The estrobolome simply gives it a name.

The Metabolic Pathway Nuance: Not All Estrogen Is Created Equal
Estrogen metabolism isn't binary. After estradiol is converted to estrone in peripheral tissues, it's further metabolized down two primary pathways:
- 2-hydroxylation → 2-OHE1: The "protective" pathway. Associated with lower proliferative activity and favorable outcomes in estrogen-sensitive tissues.
- 16-hydroxylation → 16-OHE1: The "proliferative" pathway. Associated with stronger estrogenic activity and higher mitogenic potential.
The ratio between these two metabolites matters—and the gut microbiome influences which direction the dial turns. Cruciferous vegetables support CYP1A1 enzyme activity, which favors the 2-OH pathway. Dysbiosis, chronic inflammation, and impaired detoxification can push metabolism toward the 16-OH pathway. So the question isn't just how much estrogen is circulating—it's what kind, and where it's going.
The Reproductive Years: When Your Gut Meets Your Cycle
Progesterone isn't just a fertility hormone. It's a motility hormone. Elevated progesterone in the luteal phase slows gut motility—a feature, not a bug, in terms of nutrient absorption during potential pregnancy. But when gut transit time increases, estrogen has more opportunity to be deconjugated and reabsorbed before it exits.
Add dysbiosis to that equation, and you get a pattern that looks like this:
- Heavy, clotty periods (excess estrogen thickens the uterine lining)
- Jawline and chin acne (androgenic + estrogenic drive on sebaceous glands)
- Cyclical bloating in the week before menstruation
- PMS — specifically the irritable, fluid-retaining, breast-tender variant
- Constipation in the luteal phase, which amplifies all of the above
These symptoms are not personality flaws. They are, in many cases, a gut problem wearing a hormone costume.
Perimenopause: When the Plot Really Thickens
Perimenopause doesn't start when your period stops. For many women, it starts in their late 30s—and the first thing to go is progesterone, not estrogen. Progesterone production requires a successfully ovulated egg. As ovulations become less frequent and less robust, progesterone drops while estrogen continues, creating a relative dominance that the estrobolome happily amplifies.
Then, because cortisol and progesterone compete for the same precursor (pregnenolone), chronic stress accelerates this depletion further. The result is a woman in her late 30s or early 40s who is technically "premenopausal" by any conventional definition, yet experiencing:
- 3AM waking (a classic sign of nocturnal cortisol spikes and blood sugar dysregulation exacerbated by estrogen fluctuation)
- Heightened anxiety with no identifiable external cause
- Erratic cycles—shorter, longer, heavier, lighter, all in the same year
- New onset migraines, often perimenstrually
- Brain fog that dermatologists, psychiatrists, and neurologists each claim is someone else's problem
The gut, meanwhile, is recycling estrogen overnight. Beta-glucuronidase activity doesn't keep business hours.
Menopause: The Ovaries Retire, the Gut Stays Busy
At menopause, the ovaries reduce estrogen production substantially—but they don't stop the body's relationship with estrogen entirely. Adipose tissue (fat cells) takes over peripheral estrogen production via aromatase enzyme activity, converting androgens to estrogen. The gut microbiome continues to modulate what circulates.
Here's the compounding problem: gut microbiome diversity typically declines with age (Simpson, 2003). Fewer species, less resilience, less ability to regulate beta-glucuronidase activity. Simultaneously, the estrogen that is produced becomes more influential on peripheral tissues—including the skin.
The clinical presentation of menopause-era estrogen dysregulation through the gut includes:
- Stubborn abdominal adiposity (adipose is both the estrogen source and the estrogen target)
- Accelerated skin aging — particularly collagen loss and loss of dermal thickness
- Cognitive changes driven in part by reduced estrogen's neuroprotective effects
- Mood instability that SSRIs alone rarely resolve fully
The Skin Connection: Your Estrobolome Writes on Your Face
Skin is not a passive bystander in this story. Estrogen receptors (ERα and ERβ) are expressed in keratinocytes, fibroblasts, and melanocytes. Estrogen directly stimulates collagen synthesis, maintains skin hydration, and supports wound healing. The research is precise: women lose approximately 30% of dermal collagen in the first five years after menopause (Brincat et al., 1985; Stevenson & Thornton, 2007).
Estrogen excess and estrogen deficiency produce different but equally disruptive skin presentations:
Signs of estrogen excess (often estrobolome-driven recirculation):
- Cystic, hormonal acne — particularly jawline and chin
- Hyperpigmentation and melasma
- Puffiness and fluid retention
- Oily, congested skin in the luteal phase
Signs of estrogen deficiency (menopause and post-menopause):
- Accelerated fine lines and loss of skin firmness
- Thinning, crepey skin texture
- Increased sensitivity and redness
- Delayed wound healing
Treating the skin without addressing the hormonal and microbiome context is, to put it plainly, treating the headline and ignoring the article.
The Fragmented System: Five Specialists, Zero Synthesis
Here's a pattern worth naming out loud. A woman presents with: jawline acne, heavy periods, anxiety, poor sleep, and skin that has aged noticeably in the past two years. She sees a dermatologist, a gynecologist, a psychiatrist, a sleep specialist, and a general practitioner. She leaves with five different assessments and a small pharmacy of prescriptions, none of which are talking to each other.
If three or more of the following are present, they are almost certainly one pattern, not five unrelated diseases:
- Cyclical or persistent jawline/chin acne
- Heavy, clotty, or painful periods
- Perimenstrual or perimenopausal anxiety and irritability
- Waking between 2–4AM
- Cyclical bloating or constipation
- Significant recent skin aging or collagen loss
- Brain fog, particularly in the second half of the cycle or post-menopause
The estrobolome is not the only variable in this picture—but it is a central and consistently underaddressed one.
Why a Probiotic From the Supermarket Probably Won't Fix It
Let's be direct: the microbiome does not restructure quickly, and it does not restructure with a generic 10-billion CFU capsule purchased from a pharmacy shelf.
The core microbiome is established early in life and proves remarkably resistant to rapid change. Meaningful, durable modulation of the estrobolome requires a multi-pronged approach sustained over months to years—not a 30-day probiotic course. This isn't pessimism; it's an accurate framing of the timeline that allows for realistic, effective intervention rather than repeated disappointment with supplements that were never designed for this purpose.
The intervention hierarchy, in order of impact, looks something like this:
- Remove what's driving dysbiosis (ultra-processed foods, chronic stress, antibiotic overuse, sleep deprivation)
- Rebuild microbial diversity through nutritional strategy
- Support liver phase I and II detoxification
- Introduce targeted, strain-specific probiotic support
Which Strains Actually Matter for the Estrobolome?
Strain specificity is everything in this space. Not all Lactobacillus species do the same thing; "contains probiotics" on a label is marketing, not medicine. The strains with meaningful evidence for estrobolome-relevant activity include:
- Lactobacillus acidophilus: Supports vaginal and intestinal pH, competes with beta-glucuronidase-producing bacteria
- Lactobacillus rhamnosus GG: One of the most studied strains for gut barrier integrity and immune modulation; reduces intestinal permeability that allows reabsorption of unconjugated estrogens
- Lactobacillus reuteri: Anti-inflammatory, supports the gut-brain axis, shown to influence systemic immune and hormonal markers
- Bifidobacterium longum: Supports SCFA production, improves bowel transit time (directly relevant to luteal phase constipation and estrogen recirculation)
- Bifidobacterium lactis: Enhances immune function and gut barrier; reduces systemic inflammation that dysregulates estrogen signaling
- Lactobacillus plantarum: Broad-spectrum gut barrier support; particularly useful in inflammatory gut environments
- Lactobacillus gasseri: Emerging evidence for influence on body composition, particularly abdominal fat accumulation—relevant to postmenopausal estrogen dynamics
The practical takeaway: look for multi-strain products that specify these organisms by strain designation, not just genus and species. Work with a practitioner who understands the clinical context rather than selecting supplements by star rating.
The Non-Negotiables: Lifestyle as Estrobolome Medicine
No amount of targeted supplementation compensates for lifestyle factors that continuously degrade the microbiome. The following are non-negotiable levers:
Movement: Regular moderate exercise increases gut microbial diversity and improves bowel transit time. Extreme or chronic overexercise, paradoxically, suppresses it. Aim for consistency over intensity.
Nutritional diversity: A minimum of 30 different plant foods per week is associated with significantly greater microbiome diversity (per the American Gut Project data). Fiber is the primary fuel for beneficial bacteria; cruciferous vegetables specifically support the 2-OH estrogen pathway.
Stress management: Cortisol directly alters gut permeability and microbiome composition. This is not a lifestyle recommendation—it's a mechanistic one. Chronic stress is a microbiome-disrupting event.
Sleep quality: Sleep deprivation alters gut microbiome composition within days. It also disrupts cortisol and melatonin rhythms that interface with estrogen regulation. The 3AM waking pattern is not just a symptom of estrogen dysregulation—chronic sleep disruption perpetuates it.
The Takeaway: Treat the Root, Not Just the Surface
The estrobolome is not a wellness trend. It's a well-characterized biological system with peer-reviewed mechanistic evidence, clinical parallels that medicine has acknowledged for decades, and meaningful implications for how we approach hormonal skin health, reproductive symptoms, and aging.
Integrative skin health the foundation of what we do at Amare Aesthetics, begins with understanding that the skin is a readout. Heavy periods, jawline acne, perimenopausal anxiety, accelerated collagen loss: these are not separate problems requiring separate specialists. They are often a single pattern, expressed across multiple systems, with a gut-hormone axis that deserves serious clinical attention.
If you're ready to look at the full picture—not just the surface—we'd love to be part of that conversation.
Frequently Asked Questions About the Estrobolome
What is the estrobolome, exactly?
The estrobolome is the collection of gut bacteria whose enzymatic activity—specifically, the production of beta-glucuronidase—regulates how estrogen is metabolized and recycled in the body. A healthy estrobolome supports efficient estrogen excretion. A dysbiotic one promotes recirculation of estrogen back into the bloodstream, contributing to relative estrogen excess.
How do I know if my estrobolome is affecting my hormones?
There is no single standard clinical test for estrobolome function. However, patterns of symptoms—including cyclical jawline acne, heavy periods, luteal phase bloating or constipation, 2–4AM waking, perimenopausal anxiety, and accelerated skin aging—can indicate estrogen dysregulation that has a gut-microbiome component. Comprehensive functional testing (including DUTCH hormone testing and possibly stool microbiome analysis) provides more complete information than standard serum estradiol alone.
Can probiotics fix my estrobolome?
Targeted, strain-specific probiotics can support estrobolome health—but they are not a standalone fix. Durable microbiome change requires addressing the root causes of dysbiosis (diet, stress, sleep, antibiotic use), improving gut transit time, and supporting liver detoxification pathways. A generic high-CFU probiotic without strain specificity is unlikely to produce meaningful results.
Is the estrobolome relevant in menopause?
Yes—particularly so. As ovarian estrogen production declines, peripheral estrogen from adipose tissue and the microbiome's influence on its recirculation become proportionally more significant. Gut microbiome diversity also declines with age, reducing the natural regulation of beta-glucuronidase activity. This contributes to the stubborn weight gain, brain fog, and accelerated skin aging commonly attributed to menopause.
How does the estrobolome affect skin?
Skin contains estrogen receptors in multiple cell types, including fibroblasts (which produce collagen) and keratinocytes. Estrogen excess driven by gut recirculation can cause cystic acne, hyperpigmentation, and puffiness. Estrogen deficiency—particularly post-menopause—accelerates collagen loss (approximately 30% in the first five years), reduces dermal thickness, and increases skin fragility. Addressing the estrobolome is a legitimate and evidence-based component of skin health strategy.
How long does it take to improve estrobolome health?
Realistic timelines for meaningful microbiome change are measured in months, not weeks. The core microbiome is established early in life and changes slowly in adulthood. Initial symptom improvements may be noticed within 6–12 weeks of consistent dietary and lifestyle changes combined with targeted probiotic support, but structural microbiome remodeling is a multi-month to multi-year process.
References
- Plottel, C.S. & Blaser, M.J. (2011). Microbiome and malignancy. Science Translational Medicine, 3(98), 98ps30. https://doi.org/10.1126/scitranslmed.3002394
- Prior, J.C. (2005). Progesterone as a bone-trophic hormone. Endocrine Reviews, 11(2), 386–398.
- Brincat, M., Moniz, C.J., Studd, J.W.W., et al. (1985). Long-term effects of the menopause and sex hormones on skin thickness. British Journal of Obstetrics and Gynaecology, 92(3), 256–259.
- Stevenson, S. & Thornton, J. (2007). Effect of estrogens on skin aging and the potential role of SERMs. Clinical Interventions in Aging, 2(3), 283–297.
- Simpson, E.R. (2003). Sources of estrogen and their importance. Journal of Steroid Biochemistry and Molecular Biology, 86(3–5), 225–230.